Close
Orthokeratology (ortho-k) is the temporary reshaping of the cornea. Custom-made lenses are worn overnight to provide clear vision throughout the day. Ortho-k is used to correct and slow down myopia (nearsightedness) in children, and to correct presbyopia (age-related farsightedness) in adults.
This might remind you of biology class back in high school, but we’ve laid out the basic science behind Ortho-K below. Most people believe that ortho-k lenses function as a mold to press the cornea into a new shape. Actually, the lens doesn’t even touch the cornea; it floats on a very thin tear film, utilizing gentle hydraulic forces to reshape the cornea.
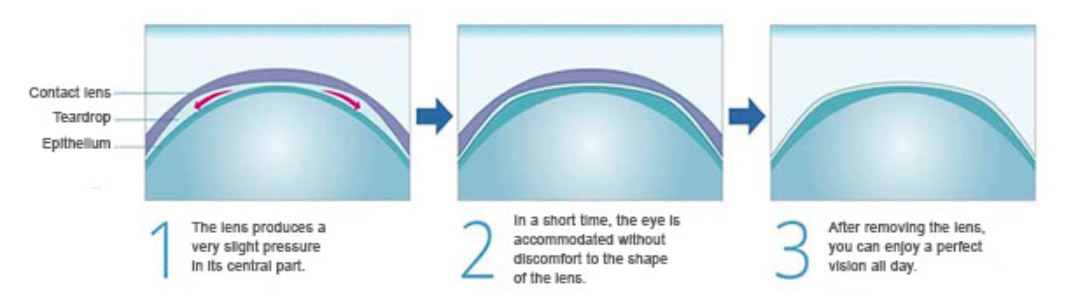
Regular contact lenses have a perfectly round dome shape. An ortho-k lens uses a reverse geometrical design in which the central area of the lens is flattened. The hydraulic forces applied to the tear film induce pressure to the center of the top tissue layer of the cornea, called the epithelium.
Because the epithelium’s cells are interconnected, the fluid they are filled with can move around between cells. When pressure is applied to the central cells, the fluid moves to the peripheral cells. As a result, the center part of the epithelium becomes thinner, and the periphery thickens.
It is important to remember that cells in the epithelium are not squished, altered, or damaged. The central cells simply undergo dehydration. After the ortho-k lens is removed, the cells gradually return to their original shape as they become hydrated again.
By flattening the cornea in this way, any nearsightedness will be corrected, resulting in perfect daytime vision. Plus, we preserve the natural state of the cornea to slow the progression of myopia.
 How Ortho-K Slows Down Myopia
How Ortho-K Slows Down MyopiaTraditional myopia correction methods only correct central vision, enabling people to see clearly at close distances. Side vision (peripheral vision), on the other hand, remains out of focus, creating what’s called peripheral hyperopia. It is generally believed that one reason for the progression of myopia is the eye’s attempt to compensate for peripheral hyperopia. By reshaping the entire cornea, blurry side vision is eliminated and the cause for elongation of the eyeball is removed.
Research studies appear to support this. The most extensive ongoing study, known as the SMART Study, found that, over a three-year period, myopia has progressed significantly less in children who wear ortho-k lenses compared to children who wear corrective eyeglasses. Previous, smaller-scale studies, such as the Kern’s Study and the Berkley’s Orthokeratology Study, produced similar results.
As early as the 1880s, a French ophthalmologist attempted to use flat-curved glass lenses to correct keratoconus by utilizing the hydraulic pressure they induced on the cornea.
In the 1950s, practitioners noticed changes in corneal curvature in some patients who wore particularly flat-fitted lenses. By this time, more compatible materials for contact lenses had been introduced. The deliberate use of modern orthokeratology began in 1962.
Although several studies proved ortho-k’s effectiveness, it wasn’t until the 1990s, when the corneal topographer was developed, that ortho-k became more widely available. Since then, the treatment has been gaining popularity. Today ortho-k is one of the preferred myopia management methodologies.